【论著】| 止吐用低频电刺激仪防治非小细胞肺癌患者化疗导致恶心呕吐的回顾性研究
时间:2023-09-19 11:07:37 热度:37.1℃ 作者:网络
[摘要] 背景与目的:晚期非小细胞肺癌(non-small cell lung cancer,NSCLC)患者接受高致吐风险的含铂双药化疗,即使采用三联或四联止吐方案,仍有相当一部分患者会出现化疗后恶心呕吐。止吐用低频电刺激仪是一种穿戴式电子止吐仪,可有效地降低各种原因引起的恶心呕吐反应,然而,在三联止吐药物的基础上联合止吐用低频电刺激仪是否可进一步提高化疗导致的恶心呕吐(chemotherapy-induced nausea and vomiting,CINV)的控制率,目前未见报道。本研究旨在评估止吐用低频电刺激仪辅助标准止吐药在应用高致吐化疗方案的NSCLC患者中的疗效和耐受性。方法:回顾性收集北京大学国际医院2019年12月1日—2022年12月30日接受一线高致吐化疗方案的晚期NSCLC患者,正确佩戴止吐用低频电刺激仪的患者作为观察组,未佩戴低频电刺激仪的化疗患者作为对照组。收集患者的临床特征、化疗后恶心呕吐发生情况,并进行患者化疗后的功能性生活指数-呕吐(functional living index-emesis,FLIE)问卷调查。采用SPSS 20.0进行统计学分析,比较两组间呕吐完全缓解率、恶心发生率和FLIE评分。结果:和对照组相比,试验组的全程无恶心率(66.3% vs 51.1%,P=0.036)和呕吐完全缓解率(83.7% vs 66.3%,P=0.006)显著提高;化疗后24~120 h的延迟期呕吐完全缓解率试验组显著提高(88.0% vs 69.6%,P=0.002),无恶心率显著提高(73.9% vs 57.6%,P=0.020)。试验组患者报告的FLIE总分和对照组患者相比差异有统计学意义(106.05±15.35 vs 95.04±20.02,P=0.020)。结论:本研究结果提示,在三联止吐方案的基础上,佩戴止吐用低频电刺激仪可改善NSCLC患者CINV的控制水平并提高患者生活质量,可作为三联止吐方案的有效补充。 [关键词] 止吐用低频电刺激仪;恶心和呕吐;化疗;非小细胞肺癌 [Abstract] Background and purpose: In patients with advanced non-small cell lung cancer (NSCLC) who receive platinum- containing dual-drug chemotherapy with high emetic risk, a significant number of patients experience nausea and vomiting after chemotherapy, even if they are treated with a triple or quadruple antiemetic regimen. The low-frequency electrical stimulator for antiemesis is a wearable electronic antiemesis device, which can effectively reduce nausea and vomiting caused by various reasons. However, no studies have investigated whether the combination of three antiemetic drugs with low-frequency electrical stimulator can further improve the control rate of chemotherapy-induced nausea and vomiting (CINV). Therefore, the aim of this study was to assess the efficacy and tolerability of low-frequency electrical stimulator for antiemesis plus standard antiemetics following highly emetogenic chemotherapy in patients with NSCLC. Methods: Data of patients with advanced NSCLC who received first-line hyperemetic chemotherapy at Peking University International Hospital from December 1, 2019 to December 30, 2022 were retrospectively collected. Patients who correctly wore low-frequency electrical stimulator for antiemesis were selected as the observation group, and chemotherapy patients who did not wear low-frequency electrical stimulator were selected as the control group. Clinical characteristics, occurrence of nausea and vomiting after chemotherapy and functional living index-emesis (FLIE) questionnaire were collected. SPSS 20.0 was used for statistical analysis to compare the vomiting complete response rate, nausea incidence and FLIE score between the two groups. Results: Compared with the control group, the no nausea rate (66.3% vs 51.1%, P=0.036) and the complete response rate of vomiting (83.7% vs 66.3%, P=0.006) in experimental group were significantly increased. At 24-120 h after chemotherapy, the complete response rate of vomiting at the delayed stage increased conspicuously in the observation group (88.0% vs 69.6%, P=0.002). At this stage, the proportion of patients without nausea in the observation group was also significantly higher (73.9% vs 57.6%, P=0.020). The total FLIE scores were conspicuously higher in the observation group than in the control group (106.05±15.35 vs 95.04±20.02, P=0.020). Conclusion: The results suggest that, on the basis of the triple antiemesis regimen, wearing the low-frequency electrical stimulator can significantly improve the control level of CINV and the quality of life of NSCLC patients, which can be an effective supplement to the triple antiemesis regimen. [Key words] Low-frequency electrical acupoint stimulation; Nausea and vomiting; Chemotherapy; Non-small cell lung cancer 化疗导致的恶心呕吐(chemotherapy-induced nausea and vomiting,CINV)是化疗患者尤为常见的不良反应之一[1],同时也是最令患者恐惧的不良反应,易造成脱水、代谢紊乱、营养失调、体重减轻,对患者的情感、社会和体力功能都会产生明显的负面影响[2]。CINV会严重影响患者的生活质量,导致患者对后续化疗依从性降低,甚至放弃可能有效但CINV较重的治疗方案,从而对患者的总生存期产生不良影响[3]。 目前,免疫检查点抑制剂治疗联合含铂药物方案成为驱动基因阴性的晚期非小细胞肺癌(non-small cell lung cancer,NSCLC)患者的一线标准治疗推荐方案。而顺铂和卡铂(AUC≥4)为高致吐风险化疗(highly emetogenic chemotherapy,HEC)药物。针对接受HEC方案的止吐治疗指南一致建议联合使用5-羟色胺-3(5-HT3)受体拮抗剂、神经激肽-1(neurokinin-1,NK-1)受体拮抗剂和地塞米松的三联止吐方案或者是联合奥氮平的四联止吐方案[4],然而即使采用三联或四联止吐方案,仍有超过1/4的患者会出现呕吐[5],恶心的缓解率更差,有52%的患者仍会出现恶心[6]。 恶心的病理生理学机制研究甚少,恶心是一种主观感觉,通常被认为是在胃中并在呕吐之前出现。目前尚不明确引起呕吐相关的神经递质和受体,如5-羟色胺和P物质,是否与恶心有关;然而,多巴胺、组胺和毒蕈碱受体可能参与其中。如何有效地缓解化疗后恶心以及进一步提高呕吐控制率是目前CINV研究的难点和热点。 P6穴,又称内关穴或G-Jo穴,位于腕掌侧远端横纹上2寸,掌长肌肌腱与桡侧腕屈肌之间。研究[7-8]认为,针刺P6穴可降低术后恶心呕吐、晨吐以及CINV的发生率和严重程度。止吐用低频电刺激仪(relief band)是根据经皮神经电刺激(transcetaneous electrical nerve stimulation,TENS)原理以及中医经络穴位理论设计的一种能有效降低由于各种原因引起的恶心呕吐反应的穿戴式电子止吐仪,通过佩戴于腕部,刺激内关穴,对缓解孕吐、手术或化疗所致恶心呕吐有显著的临床效果,于2000年获得美国食品药品管理局(Food And Drug Administration,FDA)认证,广泛应用于缓解孕吐、晕车/船、术后及化疗后呕吐等[9]。然而,在三联止吐药物的基础上联合止吐用低频电刺激仪是否可进一步提高CINV的控制率,尚未见报道。 本研究旨在评估接受高致吐风险化疗药物化疗的肺癌患者在应用标准止吐方案的基础上,辅助应用止吐用低频电刺激仪的止吐效果和不良反应。 1 资料和方法 1.1 研究设计及入排标准
本研究为一项回顾性临床研究,获北京大学国际医院伦理委员会批准(伦理批件号:2023-KY-0002-01)。入组人群为2019年12月1日—2022年12月30日接受一线高致吐化疗方案的晚期NSCLC患者,正确佩戴止吐用低频电刺激仪的患者作为观察组,未佩戴低频电刺激仪的化疗患者作为对照组。入组标准:本研究入组患者为接受单日高致吐方案(顺铂或卡铂AUC≥4)化疗的初治局部晚期或转移性NSCLC患者;经病理组织学或细胞学检查确诊;患者年龄≥18岁;采用美国东部肿瘤协作组(Eastern Cooperative Oncology Group,ECOG)PS评分,为0~1分。两组患者在化疗前均按照指南采取三联预防止吐用药方案,包括静脉注射昂丹司琼8 mg,第1~4天;静脉注射地塞米松5 mg第1天,3 mg,第2~4天;口服阿瑞匹坦120 mg,第1天,80 mg,第2~3天[4]。观察组自化疗前30 min至化疗后5 d内佩戴低频电刺激仪。低频电刺激仪由纳思科丰(大连)医疗科技有限公司提供。佩戴方法为将电刺激仪的两个金属电极贴在手腕内表面,如前述的P6穴位置。除洗澡外,患者连续佩戴该设备5 d。
1.2 数据收集
收集患者临床特征及化疗前的呕吐风险评估内容,包括年龄、性别、妊娠孕吐史、饮酒史等。收集患者化疗0~120 h呕吐发生情况、恶心发生情况、恶心严重程度。恶心的严重程度使用10 cm水平视觉模拟量表进行评估,其中0 cm表示无恶心症状,从0至10 cm恶心程度不断递增,10 cm表示恶心程度到极点。并进行患者化疗后的功能性生活指数-呕吐(functional living index-emesis,FLIE)问卷[10]调查。
1.3 统计学处理
比较两组间的急性期、延迟期和全程的呕吐完全缓解率(没有呕吐且未使用过解救药物)、恶心发生率、严重恶心发生率、FLIE评分。计量资料若符合正态分布以x±s方式表示,否则以中位数和四分位数间距表示,计数资料以百分数表示。采用Wilcoxon秩和检验和Fisher’s精确概率检验比较两组间的差异。P<0.05为差异有统计学意义。采用SPSS 20.0进行统计学分析。
2 结 果
2.1 患者特征
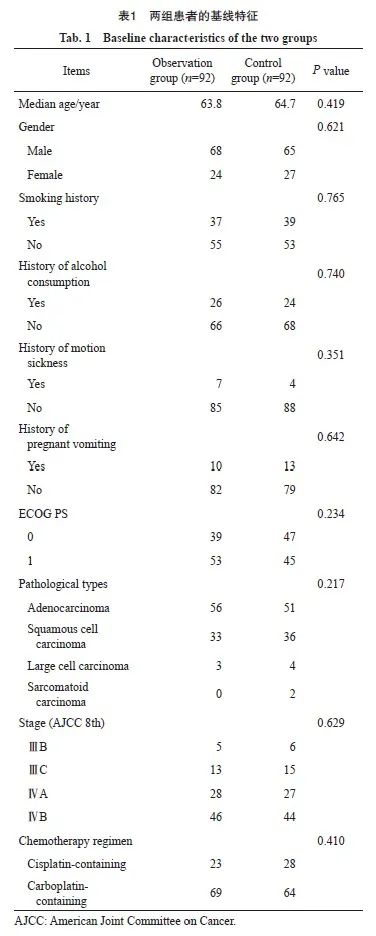
共有184例患者入组,两组各92例。患者中位年龄64岁,以男性、腺癌患者为主。除年龄、性别、病理学类型、分期匹配特征外,两组患者的基线特征均衡可比(表1)。
2.2 治疗效果
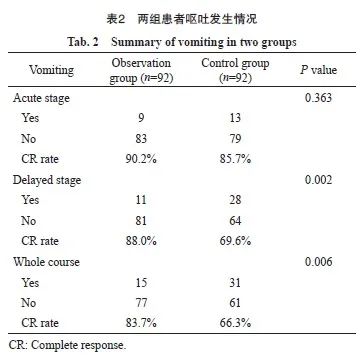
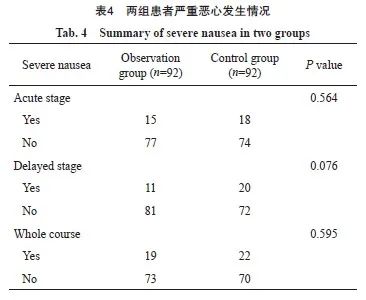
在化疗期间和化疗后的5天时间内,与对照组相比,观察组的全程无恶心率显著提高(66.3% vs 51.1%,P=0.036),全程呕吐完全缓解率显著提高(83.7% vs 66.3%,P=0.006)。在化疗后0~24 h的急性期呕吐完全缓解率(90.2% vs 85.7%,P=0.363)和无恶心率(76.1% vs 69.6%,P=0.320)两组差异均无统计学意义;化疗后24~120 h的延迟期呕吐完全缓解率实验组显著提高(88.0% vs 69.6%,P=0.002),无恶心率显著提高(73.9% vs 57.6%,P=0.020)。全程及急性期、延迟期的严重恶心发生率差异均无统计学意义(表2~4)。

2.3 生活质量评分
收集两组患者的生活质量FLIE评分,观察组患者报告的FLIE总分和对照组患者相比差异有统计学意义(106.05±15.35 vs 95.04±20.02,P=0.02)。
2.4 不良反应
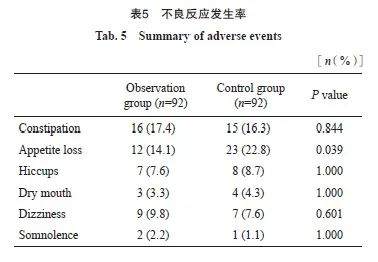
两组患者不良反应发生率,除观察组食欲下降发生率有显著下降外,其他不良反应发生率差异无统计学意义,1例观察组的患者佩戴治疗仪期间有手指刺痛,考虑为神经电刺激引起(表5)。
3 讨 论
肺癌是中国发病率和死亡率最高的恶性肿瘤,NSCLC占所有肺癌的85%[11],近20年来,多基因检测指导下的精准靶向治疗和免疫治疗显著改善了患者的预后。驱动基因阴性的晚期NSCLC,一线免疫治疗联合化疗的keynote189和keynote407研究报道患者的5年总生存率接近20%,给很多晚期肿瘤患者带来了长期生存的希望[12]。随着基因检测技术的发展,靶向治疗成为驱动基因阳性NSCLC患者的一线标准治疗并显著改善了患者的预后。对于驱动基因阴性的晚期NSCLC患者,免疫治疗的应用延长了患者的生存期,但化疗在NSCLC患者的治疗中仍占据重要地位。近年来,虽然预防性止吐治疗得到了长足发展,CINV仍然是患者最为恐惧的化疗相关不良反应[13],不仅降低患者生活质量,也影响患者的治疗依从性,从而影响预后,是临床亟待关注和解决的问题。
有研究[13]报道,呕吐反射有外周通路和中枢通路,外周通路起源于胃肠道,是由化疗药物刺激和损伤胃肠道黏膜导致多种神经递质的释放,尤其是嗜铬细胞释放神经递质5-羟色胺(5-hydroxytryptamine,5-HT)并与5-HT3受体结合,受体激活后经迷走神经向呕吐中枢传递信号,该通路主要与急性期呕吐相关;中枢机制为化疗药物直接刺激延髓化学感受器触发区,引发多种神经递质释放与受体结合,如P物质和NK-1受体,以及多巴胺及其受体等,进而刺激呕吐中枢,该通路主要与延迟期呕吐相关。随着越来越多止吐药物的研发和临床应用,化疗患者的CINV得到了很好的控制,但仍有相当一部分患者饱受CINV的困扰,尤其是接受HEC方案化疗的患者[14]。本研究发现,止吐用低频电刺激仪可显著降低NSCLC患者接受HEC方案化疗后恶心呕吐的发生率尤其是延迟期恶心呕吐的发生率,可作为三联止吐方案的有效补充。
本研究结果提示,佩戴止吐用低频电刺激仪可降低患者全程恶心和呕吐的发生率以及延迟期恶心呕吐的发生率。急性期恶心呕吐的发生率无显著改变。中医药治疗CINV疗效确切,包括针灸、穴位注射、穴位贴敷、穴位按摩、艾灸等,均可缓解化疗后的胃肠道反应[15],很多研究[15-16]证实了针灸治疗CINV的有效性,但针灸为有创操作,可能引起疼痛、感染等并发症,且需要有经验的针灸医师方可实施。因此,临床上迫切需要一种无创、方便的穴位刺激方法。P6穴位的电刺激已被证实对控制CINV有良好的效果[17]。本研究使用的止吐用低频电刺激仪是采用类似手表的佩戴方式,仅需医护人员进行简单指导患者即可妥善佩戴,十分便捷,便于临床广泛使用。本研究结果表明,在三联止吐方案的基础上佩戴电刺激仪,可降低NSCLC患者接受高致吐风险化疗的全程恶心和延迟期恶心的发生率。采用三联止吐方案虽可显著降低HEC方案化疗的呕吐发生率,但有超过一半的患者仍有恶心的发生[6],严重影响患者的生活质量,本设备的使用满足了临床的迫切需求,值得进行扩大样本量的前瞻性研究进一步验证。本研究中严重恶心发生率和急性期恶心发生率有降低趋势,但差异无统计学意义,可能与本研究样本量较小有关。
我们的研究还发现两组全程呕吐完全缓解率和延迟期呕吐完全缓解率有显著差异,再次表明本设备可改善CINV的控制。虽然急性期呕吐完全缓解率无显著差异,但二者在实验组均有改善趋势,考虑与样本量较小相关。刺激P6穴缓解恶心呕吐的机制目前尚不清楚,有研究[18]认为,低频电刺激脉冲信号经正中神经通过神经系统传递到大脑皮质,从而控制CINV的发生。总之,通过P6穴的电刺激减轻CINV发生的具体机制还需进一步研究。
本研究结果表明,佩戴电刺激仪组的FLIE评分较对照组有一定提高,可能与恶心、呕吐的发生率下降相关。本研究发现两组不良反应发生率差异无统计学意义,表明佩戴电刺激仪是安全可行的。
总之,本研究发现,在三联止吐方案的基础上,联合佩戴止吐用低频电刺激仪可改善NSCLC患者化疗后全程恶心和延迟期恶心的发生率,并提高全程呕吐和延迟期呕吐的完全缓解率,从而可改善患者化疗期间的生活质量。
利益冲突声明:所有作者均声明不存在利益冲突。
[参考文献]
[1] BARBOUR S Y. Management of patients with chemotherapyinduced nausea and vomiting[J]. J Adv Pract Oncol, 2017, 8(3): 303-308.
[2] FARRELL C, BREARLEY S G, PILLING M, et al. The impact of chemotherapy-related nausea on patients' nutritional status, psychological distress and quality of life[J]. Support Care Cancer, 2013, 21(1): 59-66.
[3] AAPRO M. CINV: still troubling patients after all these years[J]. Support Care Cancer, 2018, 26(1): 5-9.
[4] RAZVI Y, CHAN S, MCFARLANE T, et al. ASCO, NCCN, MASCC/ESMO: a comparison of antiemetic guidelines for the treatment of chemotherapy-induced nausea and vomiting in adult patients[J]. Support Care Cancer, 2019, 27(1): 87-95.
[5] GAO A, GUAN S, SUN Y, et al. Prolonged usage of fosaprepitant for prevention of delayed chemotherapy-induced nausea and vomiting (CINV) in patients receiving highly emetogenic chemotherapy[J]. BMC Cancer, 2023, 23(1): 609.
[6] WEINSTEIN C, JORDAN K, GREEN S, et al. Singledose fosaprepitant for the prevention of chemotherapyinduced nausea and vomiting in patients receiving moderately emetogenic chemotherapy regimens: a subgroup analysis from a randomized clinical trial of response in subjects by cancer type[J]. BMC Cancer, 2020, 20(1): 918.
[7] LOWN E A, BANERJEE A, VITTINGHOFF E, et al. Acupressure to reduce treatment-related symptoms for children with cancer and recipients of hematopoietic stem cell transplant: protocol for a randomized controlled trial[J]. Glob Adv Health Med, 2019, 8: 2164956119870444.
[8] WEBER B, KNOTH S, KRANKE P, et al. Study protocol for a randomised, patient- and observer-blinded evaluation of P6 acustimulation for the prevention of nausea and vomiting in the postoperative period in patients receiving routine pharmacological prophylaxis (P6NV-Trial)[J]. Trials, 2022, 23(1): 497.
[9] Reliefb and technologies[EB/OL]. [2023-04-20]http://www.reliefband.com.
[10] ALHAMMAD A M, ALKHUDAIR N, ALZAIDI R, et al. Assessing the impact of chemotherapy-induced nausea and vomiting on patients' quality of life: an Arabic version of the functional living index-emesis[J]. J Oncol Pharm Pract, 2022, 28(3): 535-541.
[11] PONS-TOSTIVINT E, BENNOUNA J. Treatments for nonsmall cell lung cancer: the multiple options for precision medicine[J]. Curr Oncol, 2022, 29(10): 7106-7108.
[12] HERBST R S, MORGENSZTERN D, BOSHOFF C. The biology and management of non-small cell lung cancer[J]. Nature, 2018, 553(7689): 446-454.
[13] GUPTA K, WALTON R, KATARIA S P. Chemotherapyinduced nausea and vomiting: pathogenesis, recommendations, and new trends[J]. Cancer Treat Res Commun, 2021, 26: 100278.
[14] PIECHOTTA V, ADAMS A, HAQUE M, et al. Antiemetics for adults for prevention of nausea and vomiting caused by moderately or highly emetogenic chemotherapy: a network meta-analysis[J]. Cochrane Database Syst Rev, 2021, 11(11): CD012775.
[15] ZHAO Y Z, DAI Y Z, NIE K. Research progress on the antiemetic effect of traditional Chinese medicine against chemotherapy-induced nausea and vomiting: a review[J]. Front Pharmacol, 2021, 12: 790784.
[16] CHEN M H, MAY B H, ZHOU I W, et al. Integrative medicine for relief of nausea and vomiting in the treatment of colorectal cancer using oxaliplatin-based chemotherapy: a systematic review and meta-analysis[J]. Phytother Res, 2016, 30(5): 741-753.
[17] CHEN B, GUO Y, ZHAO X, et al. Efficacy differences of electroacupuncture with single acupoint or matching acupoints for chemotherapy-induced nausea and vomiting: study protocol for a randomized controlled trial[J]. Trials, 2017, 18(1): 477.
[18] GARCIA G T, RIBEIRO R F, FARIA SANTOS I B, et al. Electrical stimulation of PC 6 to control chemotherapy-induced nausea and vomiting in patients with cancer: a systematic review and meta-analysis[J]. Med Acupunct, 2021, 33(1): 22-44.

