病例报告|以共济失调起病的Lambert-Eaton肌无力综合征1例
时间:2024-08-13 14:01:17 热度:37.1℃ 作者:网络
摘 要 Lambert-Eaton 肌无力综合征(Lambert-Eaton myasthenic syndrome,LEMS)是一种免疫介导的累及神经肌肉接头疾病,主要表现为肌无力、自主神经功能障碍及腱反射减低。现报告1例LEMS患者,以头晕、共济失调为首发症状,后出现眼睑下垂,重复神经电刺激可见低频递减,高频递增,P/Q型压力门控钙离子通道(voltage-gated calcium channels ,VGCC)抗体阳性,胸部CT提示肺结节及肿大纵隔淋巴结,经穿刺活检病理证实为小细胞肺癌。提示神经内科医师,共济失调也是LEMS的重要表现之一,避免漏诊。
关键词
Lambert-Eaton肌无力综合征;共济失调;压力门控钙离子通道;小细胞肺癌;氨吡啶缓释片
Lambert-Eaton肌无力综合征(Lambert-Eaton myasthenic syndrome ,LEMS)是一种免疫介导的神经肌肉接头疾病,临床三主征为短暂活动后可改善的近端肌无力、腱反射减低及自主神经功能障碍[1]。以共济失调起病的LEMS患者非常罕见[2],易误诊为自身免疫性脑炎。现报告1例以小脑型共济失调为首发症状的P/Q型电压门控钙离子通道(voltage-gated calcium channels, VGCC)阳性的LEMS患者。
1 临床资料
患者,女,60岁,因“头晕、行走不稳3.5个月,复视、闭目及四肢无力3个月余”入院。患者3.5个月前出现头晕,行走不稳,无恶心呕吐、视物旋转。3个月余前出现视物成双、双眼闭目无力,伴构音不清、双上肢抬举及双下肢蹲起费力,无晨轻暮重、眼睑下垂,无饮水呛咳、吞咽困难、口角歪斜,外院诊断为“Miller Fisher综合征”,予免疫球蛋白及甲泼尼龙冲击治疗,视物成双及构音不清缓解,行走不稳稍好转。2个月前行走不稳缓慢加重。自发病来口干,睡眠差,二便正常,体质量下降2 kg。
专科检查:双眼闭目力弱,余脑神经未见异常。四肢近端肌力5-级,远端肌力正常,四肢腱反射减低。双侧病理征未引出。深浅感觉正常。双上肢指鼻试验欠稳准,双侧反击征阳性,双下肢跟膝胫试验不稳。步基宽,走直线及单足力不能。Romberg征阴性。定时25英尺步行测试(Timed 25-foot walk ,T25FW) 4级,起立-行走计时试验(timed up to go,TUG) 39.8 s。共济失调评分(scale for the assessment and rating of ataxia,SARA):左侧12分,右侧11分,平均11.5分。新斯的明试验阴性。
辅助检查:血常规、肝肾功能正常,血沉、类风湿因子、抗核抗体、抗中性粒细胞胞浆抗体未见异常。重症肌无力抗体阴性。血清抗VGCC抗体阳性(放射免疫法)65.39 pmol/L(参考值≤30 pmol/L),抗Y染色体性别决定区相关高迁移率超家族1(recombinant sex determining region Y box protein 1,SOX1)抗体(CBA法)弱阳性,胃泌素释放肽前体(progastrin releasing peptide,ProGRP)(电化学发光法)923.10 pg/mL(参考值<69.2 pg/mL)。血和脑脊液抗Hu、Yo、Ri抗体阴性。脑脊液常规和生化正常。重复神经电刺激可见低频(3~5 Hz)递减(17.7%~29.5%),高频(30 Hz)递增(111.3%),10 s大力运动即刻波幅较运动前增高107%。肌电图:四肢神经运动传导波幅减低,双下肢皮肤交感反射(sympathetic skin response,SSR)异常。头核磁未见明显异常。胸部CT平扫增强示右肺下叶结节、纵隔淋巴结肿大,呈不均匀强化。18F-FDG PET-CT提示右肺下叶恶性病变伴纵膈淋巴结转移可能性大(图1)。
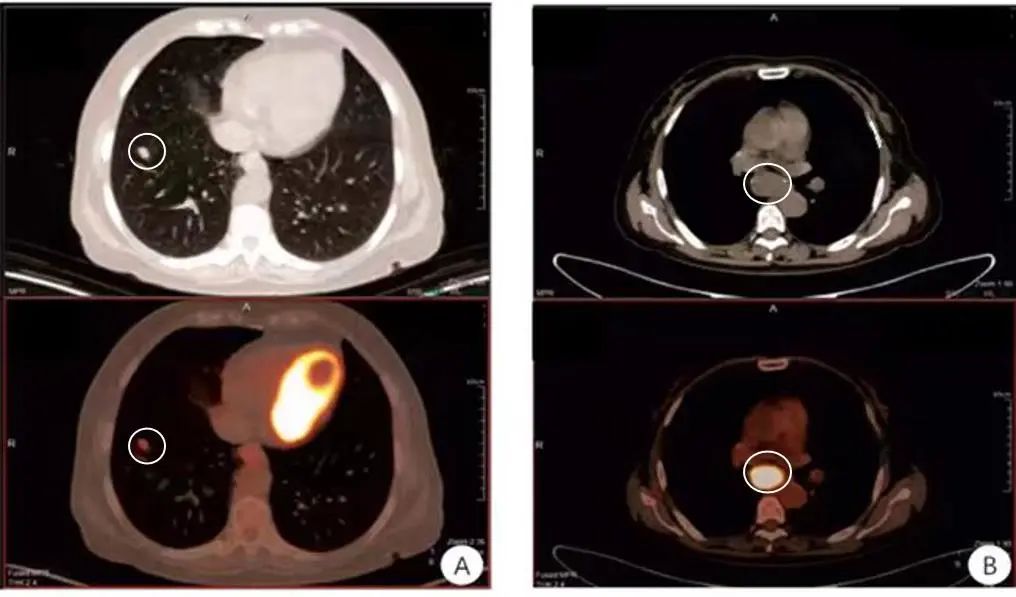
图1 18F-FDG PET-CT 示右肺下叶前基底段放射性摄取增高(SUVmax 2.81 ,A),纵隔肿大淋巴结放射性摄取明显增高(SUVmax 13.61 ,B)Fig.1 18F-FDG PET-CT showed increased radioactive uptake in the anterior basal segment of the right inferior lobe (SUVmax 2.81, A), and significantly increased radioactive uptake in the enlarged mediastinal lymph nodes (SUVmax 13.61, B)
予氨吡啶缓释片(10 mg,每日两次)口服,服药3 d后双下肢共济失调症状改善:SARA评分左侧9分,右侧8分(指鼻、轮替和跟膝胫试验好转),平均8.5分;T25FW 4级,TUG 34 s;临床总体改善印象量表评分3分,稍好转;主观疗效总体评分3分,轻度改善。行纵隔淋巴结活检术,纵隔第7组淋巴结病理回报为小细胞肺癌(图2),行依托泊苷、卡铂化疗。出院1个月后,电话联系患者,诉可自行缓慢行走。最终诊断:Lambert-Eaton肌无力综合征,右肺下叶小细胞肺癌伴纵隔淋巴结转移。
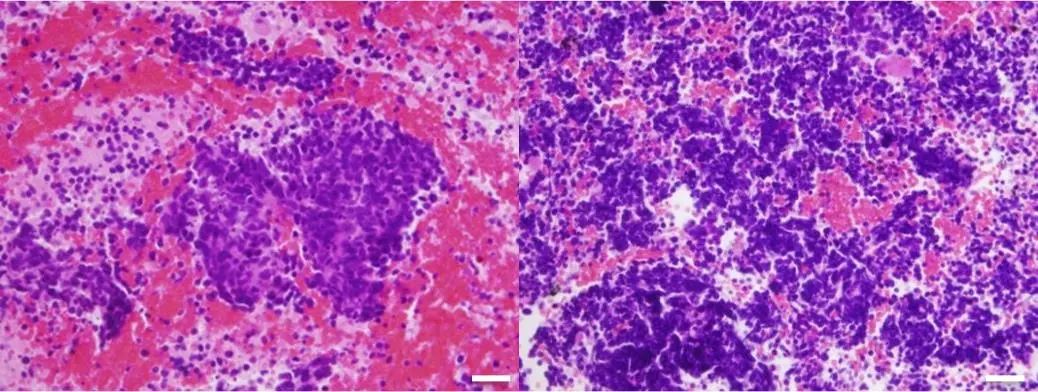
图2 纵隔肿物穿刺活检病理,HE染色(HE×400)可见部分异形细胞呈片状生长,细胞胞质稀少,形态较一致,比例尺50 μmFig.2 Pathology of mediastinal mass by needle biopsy showed flaky growth of some heteromorphic cells with sparse cytoplasm and relatively consistent morphology
2 讨论
1957年Eaton和Lambert首次报告了LEMS,2017年一项基于美国退伍军人的流行病学研究发现LEMS发病率为2.6/100万[3]。约 85%~90% LEMS患者血清P/Q型VGCC抗体阳性,该抗体与神经肌肉接头、交感和副交感神经突触前膜的VGCC结合,阻滞钙离子内流,突触前膜Ach囊泡释放减少,导致肌无力和自主神经功能障碍[4]。自主神经症状以口干最常见,此外男性勃起功能障碍、便秘、排尿困难多见,眼干、体位性低血压、排汗困难、头晕等相对少见[2, 5]。
LEMS根据是否合并肿瘤,分为副肿瘤性和自身免疫性两种亚型。小细胞肺癌(small-cell lung carcinoma ,SCLC)是副肿瘤性LEMS主要病因,占LEMS总数50%~60%,几乎所有合并SCLC的LEMS患者可检出P/Q型VGCC抗体阳性[6]。临床上常用LEMS肿瘤相关预测评分( Dutch-English LEMS Tumor Association Prediction Score ,DELTA-P评分) 判断 LEMS 合并肿瘤的概率,当评分≥3分时肿瘤风险显著增加,评分越高,肿瘤风险越高[7]。
P/Q型VGCC在小脑平行纤维-浦肯野细胞的突触传递中也发挥重要作用[8],在副肿瘤引起小脑变性的患者中观察到小脑中P/Q型VGCC较对照组减少70%~80%,推测VGCC减少可引起小脑共济失调[9]。一项总结97例LEMS患者临床表现的研究,也报道了副肿瘤性LEMS出现小脑型共济失调[2]。
此外,该患者抗SOX1抗体弱阳性,抗SOX1抗体能特异性结合小脑浦肯野细胞层Bergmann星形胶质细胞核[10],导致小脑功能异常,也可能是小脑共济失调的原因之一。抗SOX1抗体阳性往往提示SCLC的可能,一项纳入520例抗SOX1抗体阳性患者的研究[11]发现,93.5%患者有肿瘤,其中SCLC占85.2%。ProGRP也是SCLC的标志物之一,用以鉴别SCLC与非小细胞肺癌[12]。该患者抗SOX1抗体弱阳性、ProGRP增高,高度提示SCLC,最终纵隔淋巴结病理证实。
在LEMS中,应用钾离子通道阻断剂阻滞突触细胞前膜的钾离子通道,使钙离子通道开放时间增多,释放更多的乙酰胆碱,可以改善肌无力症状[13]。氨吡啶是广谱的钾离子通道阻滞剂,改善肌无力的同时还可增加小脑浦肯野细胞的兴奋性,解除GABA对小脑的抑制作用[14],进而减轻小脑共济失调。本例患者服用氨吡啶缓释片3 d后TUG改善14.7%,SARA评分改善25%。
本例患者起病初期表现共济失调,出现眼睑闭合及四肢近端无力后才考虑是否为神经肌肉接头疾病,因此神经内科医生能认识到共济失调也是LEMS的重要表现之一,可以提高确诊率。
参考文献:
1. KESNER V G, OH S J, DIMACHKIE M M, et al. Lambert-Eaton Myasthenic Syndrome[J]. Neurol Clin, 2018, 36(2): 379-394.
2. TITULAER M J, WIRTZ P W, KUKS J B, et al. The Lambert-Eaton myasthenic syndrome 1988-2008: A clinical picture in 97 patients[J]. J Neuroimmunol, 2008, 201-202: 153-158.
3. ABENROTH D C, SMITH A G, GREENLEE J E, et al. Lambert-Eaton myasthenic syndrome: Epidemiology and therapeutic response in the national veterans affairs population[J]. Muscle Nerve, 2017, 56(3): 421-426.
4. VINCENT A. Immunology of disorders of neuromuscular transmission[J]. Acta Neurol Scand Suppl, 2006, 183: 1-7.
5. WIRTZ P W, SMALLEGANGE T M, WINTZEN A R, et al. Differences in clinical features between the Lambert-Eaton myasthenic syndrome with and without cancer: an analysis of 227 published cases[J]. Clin Neurol Neurosurg, 2002,104(4):359-363.
6. GUIDON A C. Lambert-Eaton Myasthenic Syndrome, Botulism, and Immune Checkpoint Inhibitor-Related Myasthenia Gravis[J]. Continuum (Minneap Minn), 2019, 25(6): 1785-1806.
7. TITULAER M J, MADDISON P, SONT J K, et al. Clinical Dutch-English Lambert-Eaton Myasthenic syndrome (LEMS) tumor association prediction score accurately predicts small-cell lung cancer in the LEMS[J]. J Clin Oncol, 2011, 29(7): 902-908.
8. WESTENBROEK R E, SAKURAI T, ELLIOTT E M, et al. Immunochemical identification and subcellular distribution of the alpha 1A subunits of brain calcium channels[J]. J Neurosci, 1995, 15(10): 6403-6418.
9. FUKUDA T, MOTOMURA M, NAKAO Y, et al. Reduction of P/Q-type calcium channels in the postmortem cerebellum of paraneoplastic cerebellar degeneration with Lambert-Eaton myasthenic syndrome[J]. Ann Neurol, 2003, 53(1): 21-28.
10. SABATER L, TITULAER M, SAIZ A, et al. SOX1 antibodies are markers of paraneoplastic Lambert-Eaton myasthenic syndrome[J]. Neurology, 2008, 70(12): 924-928.
11. SUN X, TAN J, SUN H, et al. Anti-SOX1 Antibodies in Paraneoplastic Neurological Syndrome[J]. J Clin Neurol, 2020, 16(4):530-546.
12. KORSE C M, HOLDENRIEDER S, ZHI X Y, et al. Multicenter evaluation of a new progastrin-releasing peptide (ProGRP) immunoassay across Europe and China[J]. Clin Chim Acta, 2015,438: 388-395.
13. SANDERS D B, JUEL V C, HARATI Y, et al. 3,4-diaminopyridine base effectively treats the weakness of Lambert-Eaton myasthenia[J]. Muscle Nerve, 2018, 57(4): 561-568.
14. MEHTA A R, KENNARD C. The pharmacological treatment of acquired nystagmus[J]. Pract Neurol, 2012, 12(3): 147-153.
【引用格式】陆慧,张冰雪. 以共济失调起病的Lambert-Eaton肌无力综合征1例[J]. 中国神经精神疾病杂志,2024,50(4):236-238.
【Cite this article】LU H,ZHANG B X. A case of Lambert-Eaton myasthenia syndrome with the onset of ataxia[J]. Chin J Nervous Mental Dis,2024,50(4):236-238.
DOI:10.3969/j.issn.1002-0152.2024.04.007

