转移性前列腺癌放射治疗的靶区勾画
时间:2023-01-15 12:01:40 热度:37.1℃ 作者:网络
转移性前列腺癌放射治疗适应证
1、区域淋巴结转移,首选放射治疗联合ADT。
2、初诊为局限期,经根治性手术或放射治疗后进展,出现新发转移灶,针对转移灶行局部放疗,同时配合全身药物治疗。
3、初诊即有远处转移,但转移灶数目较少,为寡转移(≤5处),可在ADT 基础上尽早行原发灶放疗,可改善预后。
4、初诊为多发转移,但有症状的患者,如因原发灶引起尿频、尿急、尿痛、尿道梗阻、血尿和直肠压迫症状,以及转移灶引起脊髓压迫、压缩性骨折和疼痛,可行减症放疗。
转移性前列腺癌靶区勾画
01
体位固定
根据转移灶不同的位置进行定位。
1、腹盆部
仰卧于全身体架上,双手上举抱肘置于额前,热塑膜成形体膜固定中下腹部(或选择其他固定方式)。
2、胸部
仰卧于全身体架上,双手上举抱肘置于额前,热塑膜成形体膜固定胸部(或选择其他固定方式)。
3、颈部
仰卧于全身体架上,双手放于身体两侧,热塑膜成形颈肩膜固定头颈部(或选择其他固定方式)。
02
CT扫描
根据转移灶位置进行。
目前国内最常采用的定位方式是CT定位。
扫描转移灶所在范围为CT 层厚3~5mm。
对于肋骨转移灶、肺内转移灶等受呼吸影响较大的病灶,建议行4D-CT扫描。
03
靶区勾画
1、前列腺原发灶
靶区勾画参考根治性放疗靶区,原则上仅针对影像学可见病灶进行治疗,不推荐盆腔淋巴结引流区预防性照射。若盆腔多发转移淋巴结,建议对盆腔行预防照射。
2、转移灶
参考已有的影像学检查CT、MRI、PET/CT勾画转移灶GTV。有条件者可使用MIMI TM软件将PET/CT与CT定位图像行形变配准和融合,在精确勾画转移灶方面有明显优势,如图1、图2。

图1 前列腺原发灶和转移灶剂量分布图
前列腺原发灶:70Gy/25f;骨盆转移灶:70Gy/25f;
胸椎转移灶:60Gy/20f;椎板病灶:40Gy/20f。
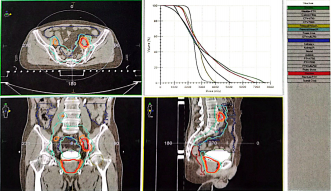
图2 前列腺原发灶和腹盆腔淋巴结转移灶放疗计划及DVH
前列腺原发灶:70Gy/25f;淋巴结转移灶:70Gy/25f;
盆腔淋巴引流区:47.5Gy/25f。
参考文献:
[1]ZAORSKY N G,PALMER J D,HURWTIZ M D. et al. What is the ideal radiotherapy dose to treat prostate cancer? A meta-analysis of biolgically equivalent dose escalation.Radiotherapy and oncology:journal of the European Society for Therapeutic Radiology and Oncology.2015, 115(3):295-300.
[2]BOEVE LS,HULSHOF M,VIS A N,et al. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patientswith Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial:Data from the HORRAD Trial. European urology. 2019,75(3):410-418.
[3]PARKER C C,JAMES N D,BRAWLEYC D,et al.Radiotherapy to the primary tumour for newly diagnosed,metastatic prostate cancer(STAMPEDE):a randomised controlled phase 3 trial.Lancet.2018,392(10162):2353-2366.
[4]PALMA D A,OLAON R,HARROW S,et al.Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers:Long-Term Results of the SABR-COMET Phase Ⅱ Randomized Trial.Journalof clinical oncology: official journal of the American Society of Clinical Oncology.2020,38(25):2830-2838.
[5]PALMA D A,OLAON R,HARROW S,et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers(SABR-COMET):a randomised,phase 2,open-labeltrial.The Lancet.2019,393(10185):2051-2058.
[6]PALMA D A,OLAON R,HARROW S,et al. Stereotactic ablative radiotherapy for the comprehensive treatment of 4-10 oligometastatic tumors(SABR-COMET-10):study protocol for a randomized phase Ⅲ trial.BMC cancer.2019,19(1):816.
[7]OLSON R,MATHEWS L,LIUM,et al. Stereotactic ablative radiotherapy for the comprehensive treatment of 1-3 Oligometastatic tumors(SABR-COMET-3):study protocol for a randomized phase Ⅲ trial.BMC cancer.2020,20(1):380.
: , 。 视频 小程序 赞 ,轻点两下取消赞 在看 ,轻点两下取消在看

